A NEW CONCEPT IN IMPLANT DENTISTRY
A “Placeholder” provisional dental implant designed for easy insertion and removal at will. The TADplant preserves crestal bone and implant sites until the patient can afford or has matured to have a standard dental implant placed.
You may be interested in reading the patent applications for a more detailed description of the TADplant and TAD Abutment. The TADplant fixture (implant part) and the abutment (Crown Support part) are described in the two patents below.
USA Patent PDF Files (Click Links)
US9629696#1 April 25, 2017 Award Date
US9980792#2 May 29, 2018 Award Date

TADplants are analogous to the “Post-it Note” developed by 3M Company. The TADplant gently integrates with the patient’s bone as a Post-it Note gently sticks to any surface. When both are removed there is no damage to the underlying surfaces.

This image is a cone beam computed tomographic rendering (CBCT) used for TADplant diagnosis and treatment planning. The TADplant is precisely positioned by the doctor. With this information a surgical guide is 3D printed for use during insertion of the TADplant. Images in the lower 2nd row illustrate the Orthoveneer system. Orthoveneers and orthocrowns are designed in computer software (CAD) with orthodontic attachments on labial or front surfaces of a tooth. Orthodontic wires will be used to move teeth into pre-planned positions.
To Launch the 3:16 min TADplant Instructional Video on your phone or other mobile device use a QR Reader Appto read the QR IMAGE below:

The video above is one of three short instructional videos. Many new dental procedures require extensive and expensive certification courses. As a Doctor you will not have to spend $5000 or more to take courses to learn how to place TADplants. As a licensed dentist or specialist, you will easily understand the flapless non-invasive insertion and removal protocols. Orthodontists and their dental colleagues have been placing and removing TADs aka “Temporary Anchorage Devices” for more than 25 years. TADs have the unique characteristic of being easily placed and removed without harming implant receptor sites. Dr. O developed and clinically tested this technique over the last 7 years. His main goals were to make the procedure super easy and affordable for patients and doctors.
The following is a summary of the Video’s content:
- First 60 seconds Fast Tracks the TADplant Insertion and Removal procedures.
- Next 60 seconds is a live surgery narrated by Dr. O as he is manually inserting two TADplants
- Last 60 seconds is an animation of how to insert TADplants with a surgical guide and motorized insertion
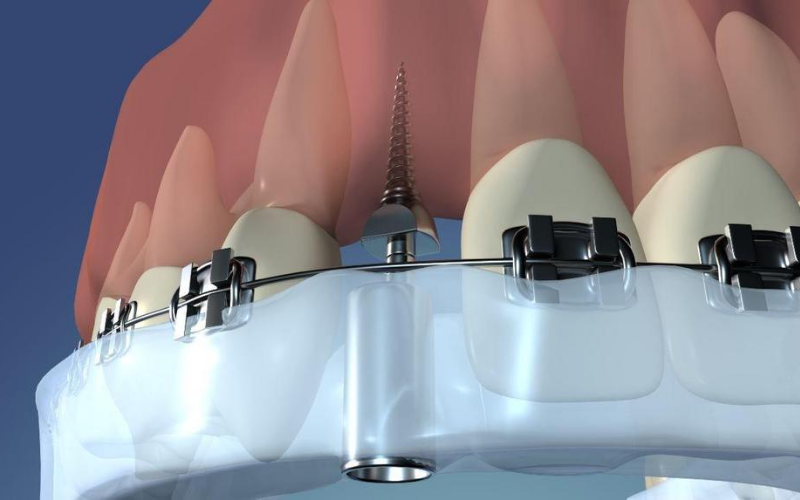
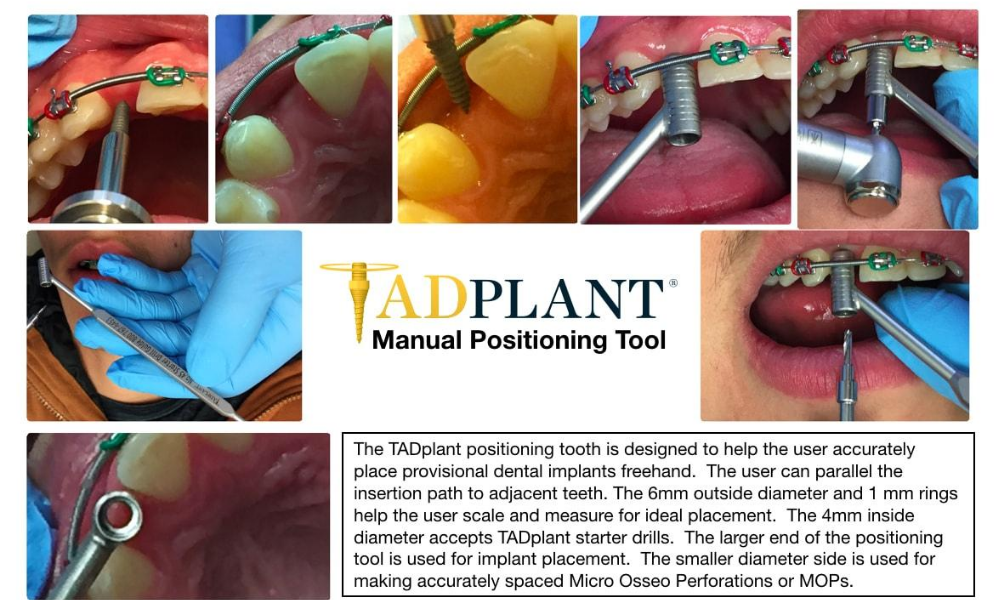
TADplants can be placed with surgical guides or free-hand by the Doctor. Our patient, Kylie’s video above was fast framed to show the TADplant protocol in 1:21 min. The image below shows the surgical guide in place that allows the Doctor to precisely place a TADplant without injuring adjacent teeth. The TADplant plus attached 6mm abutment are placed together through the guide sleeve embedded in the plastic guide. The straight abutment has 1 mm rings that help with scaling and measuring insertion depths. When a progress periapical image is taken the straight abutment mm rings can be used to scale the x-ray. The 6 mm straight abutment is also used to parallel multiple TADplant placements.
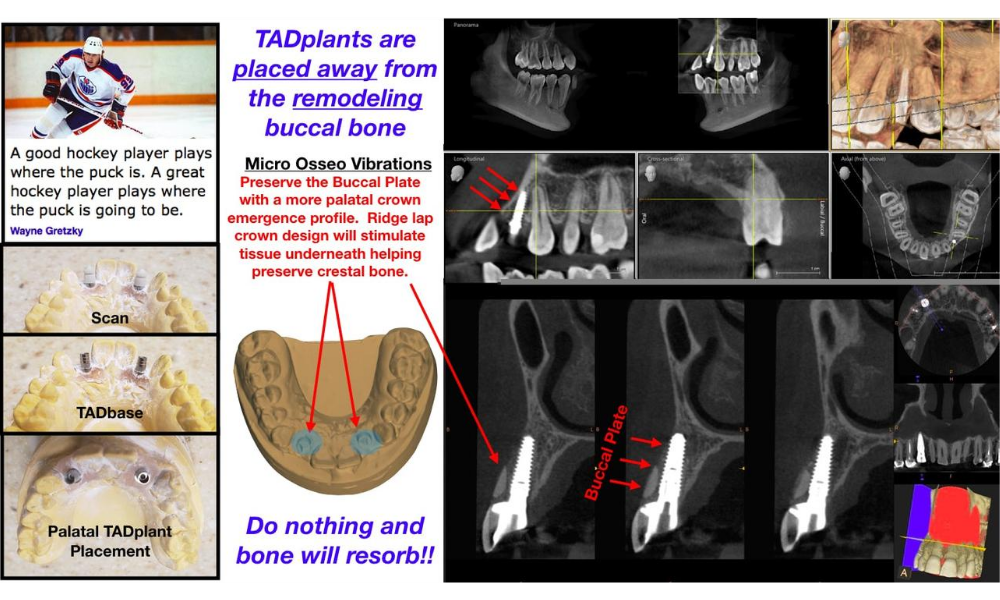
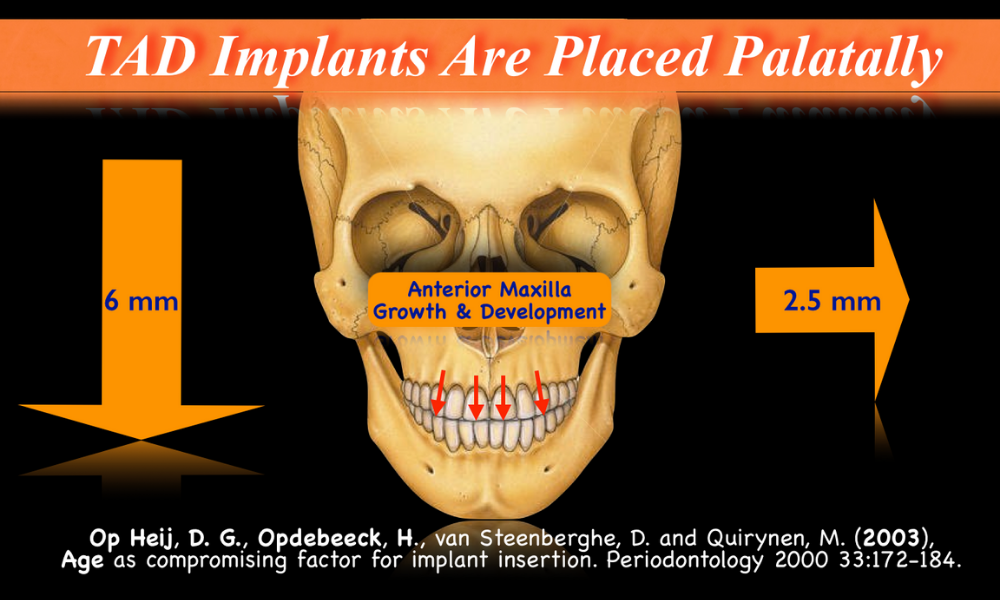
Growth and aging changes can make the maxilla a “moving target”. Provisional implants should be placed away from the buccal cortical bone. TADplant crowns are designed to protect the buccal plate. The maxilla will move 6mm downward and 2mm backward. This will vary from patient to patient. Plan for it! Avoid future complications.


Younger patients mature and bone remodels. Older patients age and bone resorbs. NORMAL expected bony changes must be considered when placing permanent dental implants at all ages.
Reference: Mendleson, Bryan and Wong, Chin-Ho, Changes in the Facial Skeleton with Aging: Implications and Clinical Applications in Facial Rejuvenation, Aesthetic Plastic Surgery, 36 (4): 753-760.
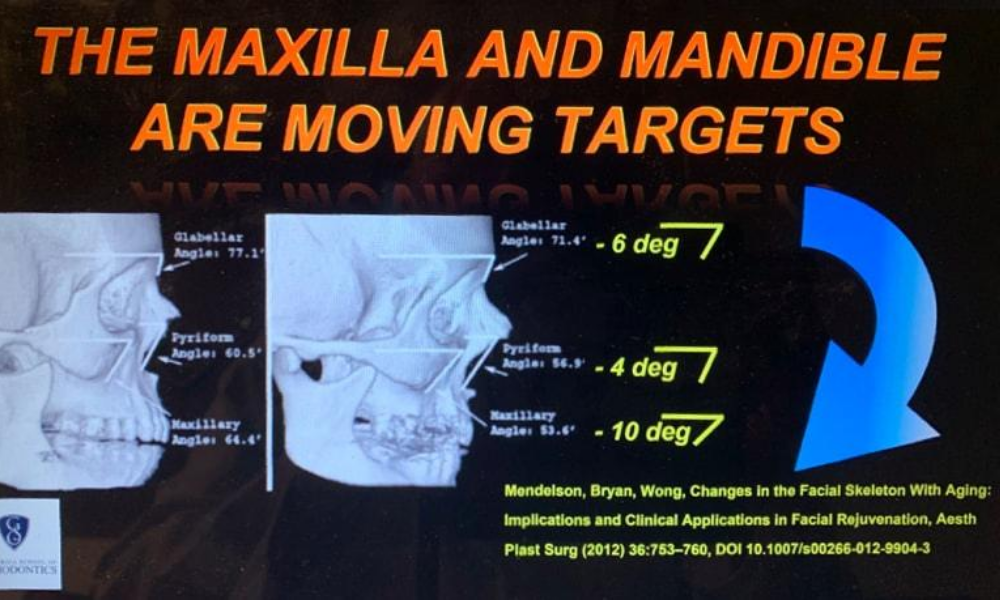
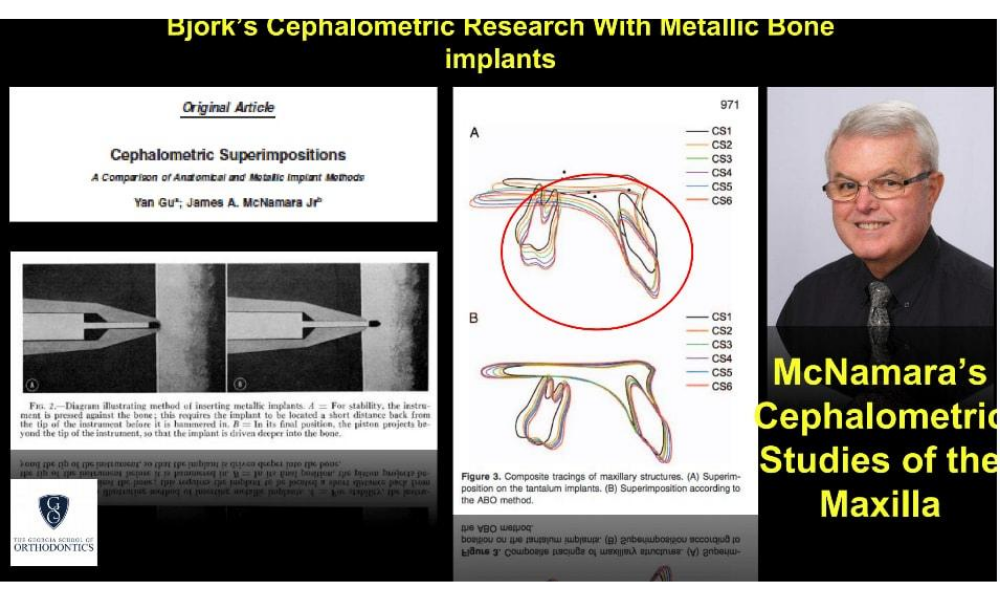
The image above is evidence of how much change occurs in the maxilla because of NORMAL growth and development. Conventional ABO-American Board of Orthodontics cephalometric superimpositions are not accurate. Yan and McNamara in their 2008 Angle Orthodontist article compare metalic pins (implants) for serial radiograph superimpositions. Their method revealed substantially more change compared to ABO anatomical landmark superimpositions. One must take the above into consideration when placing dental implants in the “Esthetic Zone”. The maxilla is a moving target!

TADplants are placed with surgical guides as illustrated above or without guides using a paralleling guide tool shown below.

When designing the TADplant I studied previous dental implant designs. Per-Ingvar Branemark is the father of modern implant dentistry. His original dental implants were machine finished with no surface enhancements. TADplants are designed exactly the same. My 95 year-old mother had original Branemark type dental implants placed in the 1980s. Her dental implants lasted for more than 30 years. When I was taking the Maxi Implant residency my mentor and instructor Dr. Ed Mills of Atlanta replaced her original implants with more modern surface enhanced dental implants. The eleven dental implants he placed are still firmly in her bone supporting her dentures. If Branemark machine finished implants lasted for more than 30 years, the TADplant could theoretically last as long. However, the TADplant will, in most cases, be removed sooner to be replaced with larger surface-enhanced dental implants.
Original TADplant concept drawing in 2010 created when taking the AAID Maxi Course
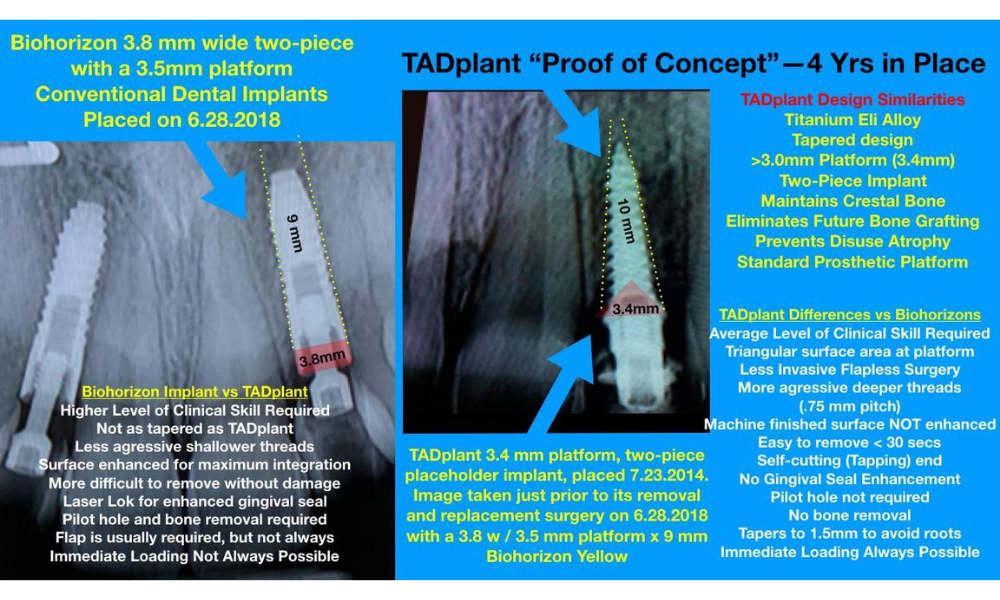
“Proof of Concept”
TADplant Provisional Implants preserved crestal bone for 4 Yrs.
Biohorizon Implants shown below placed by Dr. Jonathan Ouellette
We recently located one of first clinical trial patients in Spokane, Washington
Our patient Byron has two TADplants and provisional crowns still in place for 7 years
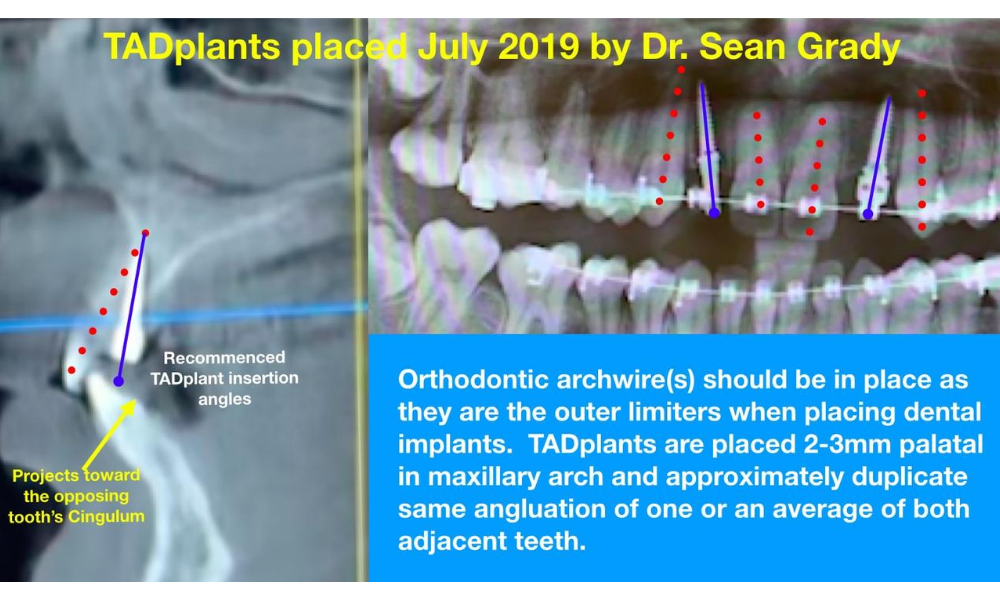
TADplant case by Doctor Sean GradyJohns Creek-Atlanta, Ga July 2019

Thank you to Tatum Surgical for helping me design the TADplant!
First Place Presentation Award at the 2012 ICOI Winter Meeting – International College of Implantology (of 54 Presenters). Dr. Ouellette has taught orthodontic residents, orthodontists, implant dentists and dental laboratory colleagues about 3D Digital Dentistry for more than 10 years.
TADplant Clinical Trials


TADplant in one of our clinical trial patients is illustrated in the image below. The TADplant mini screw implant can be placed anywhere in the mouth to preserve crestal bone. TADplants have a universal 3.4 mm (width ) prosthetic platform that is not too large or too small to support a provisional crown. We recommend placing crowns out of occlusion, not heavily touching the opposing tooth. Most implant crowns are routinely placed in “infra-occlusion”. This minimizes direct biting and lateral forces on the implant and crown. All teeth have periodontal ligaments that control functional forces to protect the teeth. A dental implant does not have a protective periodontal ligament.
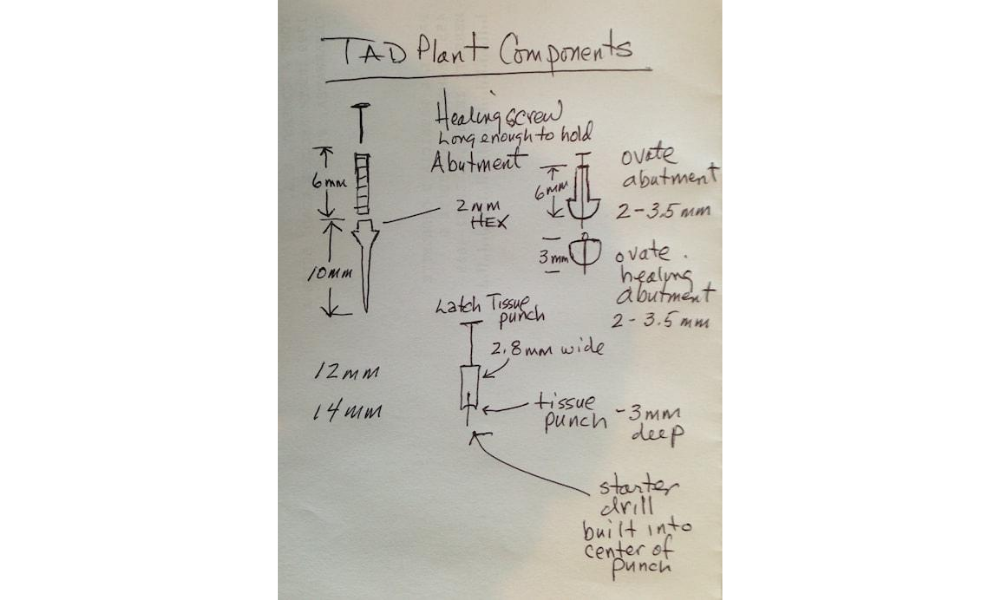
The images illustrates the TADplant’s unique design. At the crestal zone area the TADplant is much wider/larger than at the radicular/root area of the implant. The TAD fixture is designed to provide a larger surface area for bone contact in the denser cortical plate area (2-3mm under platform). The root area of the fixture then dramatically tapers to safely fit between the roots of adjacent teeth.
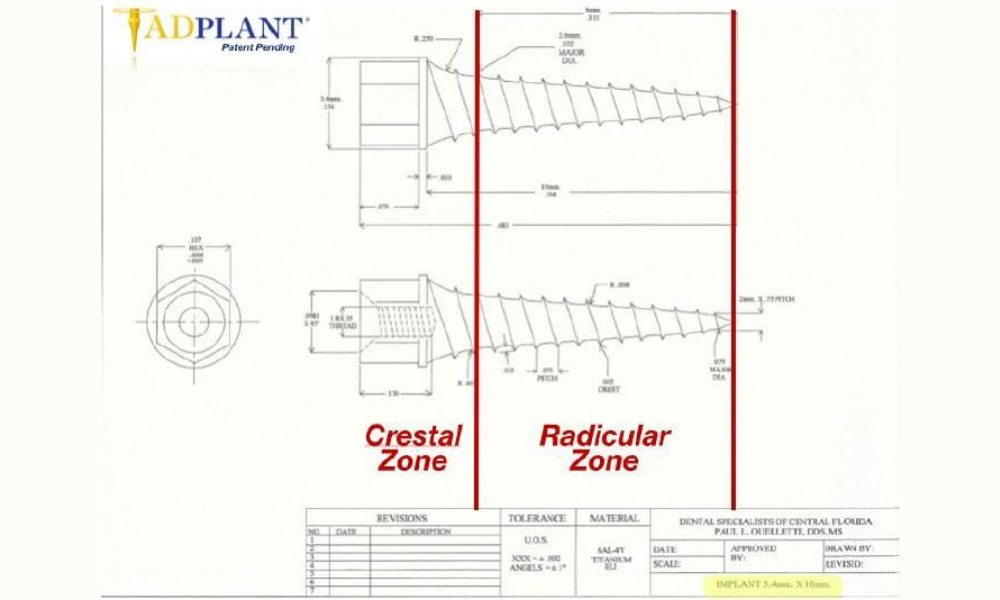
The image above is the original engineering drawing of the 10 mm long x 3.4 mm wide TADplant. Note the two zones. The Crestal Zone has the “Prosthetic Platform” with a 2 mm high external hex designed for easier removal of the dental implant. The industry standard for external hex implants is 1 mm. The Radicular Zone tapers to 1.5 mm for safe insertion without touching adjacent tooth roots.
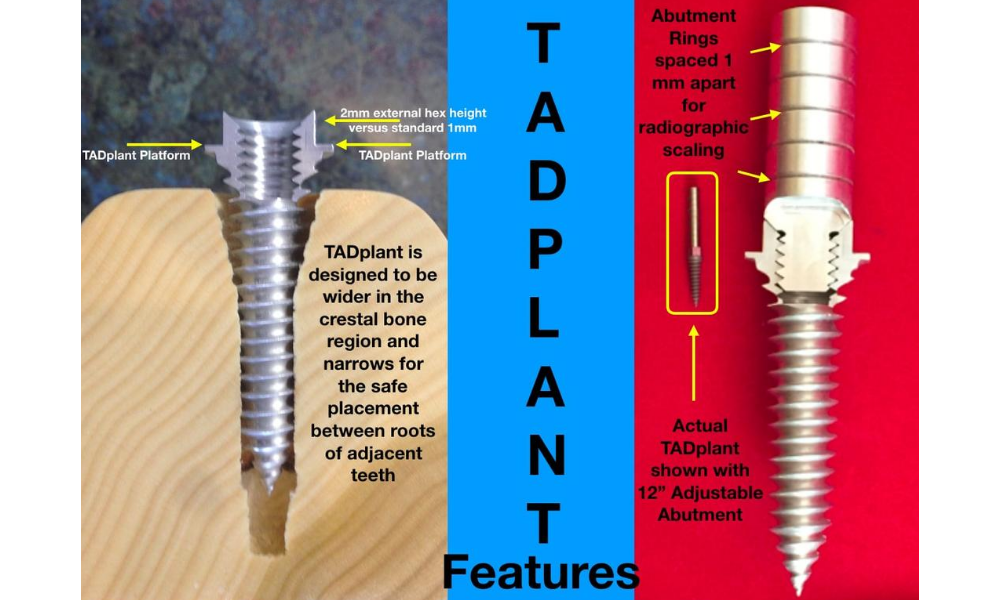
The TADplant prototype model to the right of a TADplant with a 12 mm long abutment screw. The TADplant image to the left is 10 mm long. The 10 mm TADplant is the most universally used fixture. TADplants are available in 4 mm, 6 mm, 8 mm , 10 mm and 12 mm lengths. All TADplant fixtures have the 3.4 mm prosthetic platform (part that holds the crown).

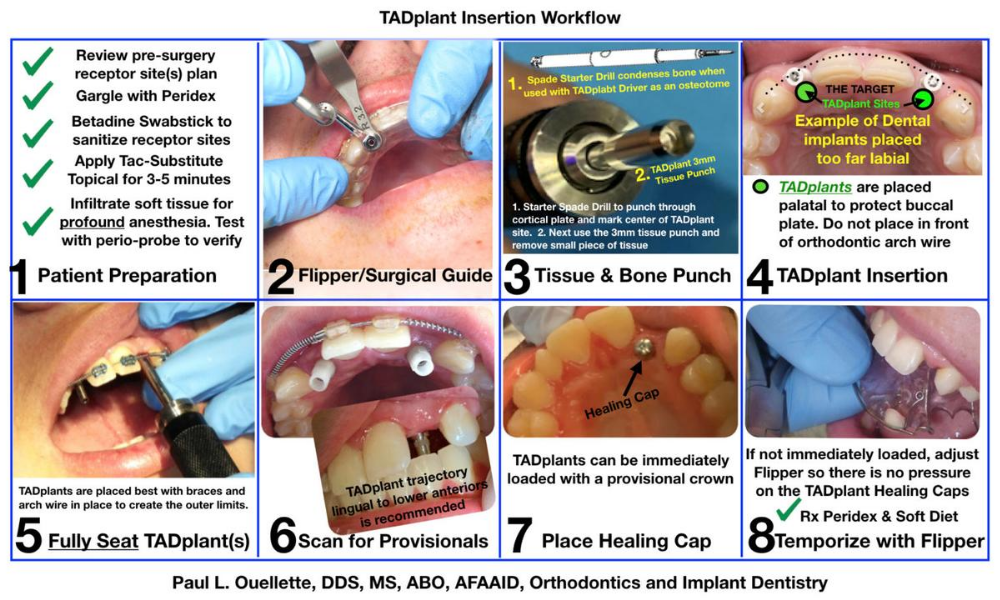
TADplant Workflow
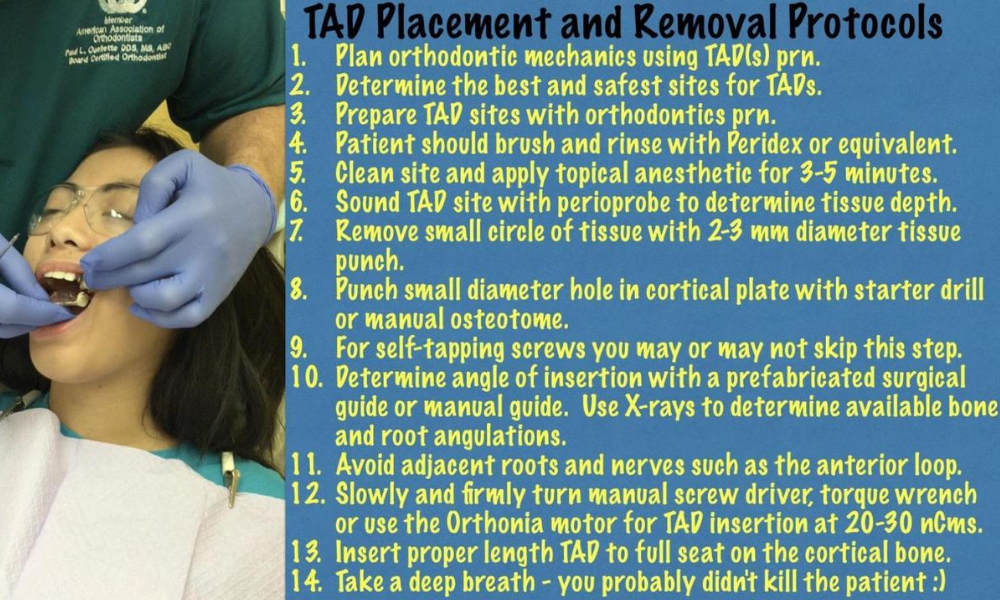
TADplant Insertion Instructions
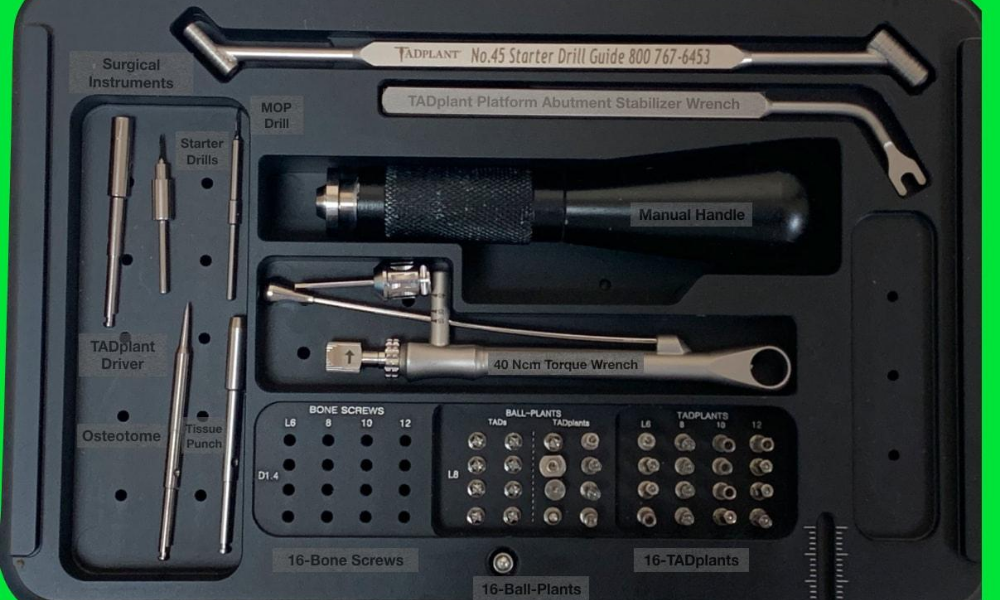
The 8-step TADplant Surgery Protocol is provided as a laminated card and a 4 x 6 water proof label affixed to the inside lid of the starter surgical kit. There are several insertion and removal videos available for review before or during the non-invasive surgical procedures. Use the QR Code provided below to access the 3-minute insertion / removal instructional video.

Evidence Based Orthodontics and Implant Dentistry
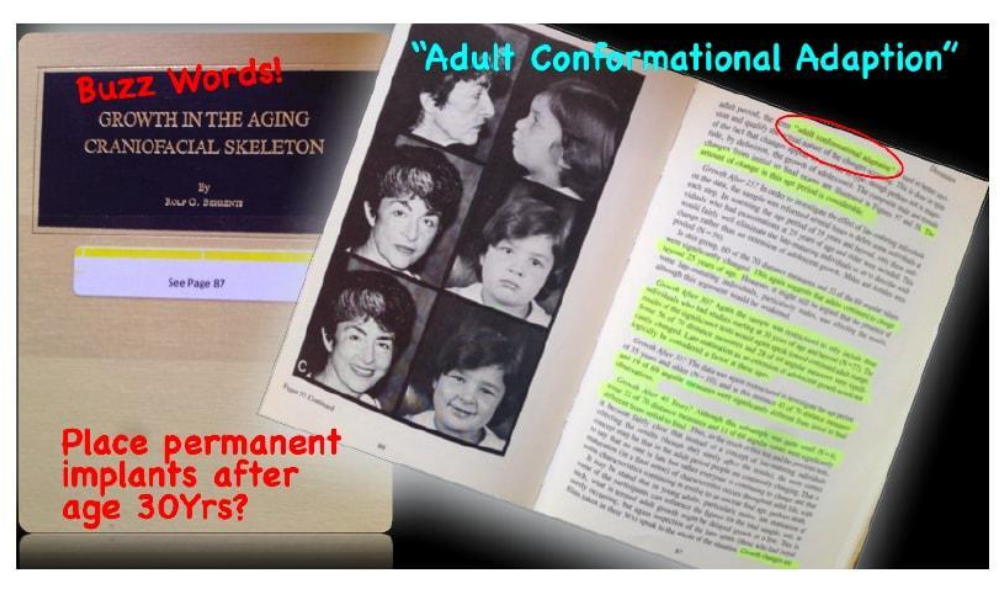
Orthodontists study in depth growth and development as part of their specialty training. A landmark study, by Dr. Rolf Behrents aka Buzz, Editor of the American Journal of Orthodontics documents growth changes in the maxillary and mandible. Dr Behrents describes, “Adult conformational changes” on page 87, that can adversely affect long term stability of dental implants placed in younger patients. Aging changes) after 40 may also affect implant stability. (ref: Bahat, Oded., Dynamic Craniofacial Changes Associated with Aging. Vumedi, Jul 21, 2015). Taking into consideration NORMAL development changes of the maxilla (upper jaw), implant dentists may consider using a dental implant that does not super-integrate in the bone. The anterior maxilla (upper jaw) grows an average of 6 mm downward and 2 mm backward in the esthetic zone (upper front teeth). The crestal area of the maxilla can move backward or towards the palate two or more millimeters. Because of these changes, a crown will appear to be higher than the adjacent teeth (infra-occlusion) and metal threads of the implant may be exposed showing through the gum tissue above the crown. Permanent dental implants may be placed more anterior (versus an initial palatal position) with less risk after most of the bone development changes described above at age 30 on to the 40s.
The TADplant system has been in development since year 2010. More than 30 components have been developed for the TADplant System. New components are being developed for treatment of sleep apnea. My friend and colleague Dr. Sam Callender developed an implant supported concept for advancing the lower jaw in apnea patients. TADplant System components are designed to be soft tissue friendly and would be well suited for his application. Clinical trials will be done in the near future at one of the orthodontic residency programs.
Click link > https://tadplant.com/tadplant-component-list-compressed/
TADplant and Orthoveneer/OrthoCrown Workflows
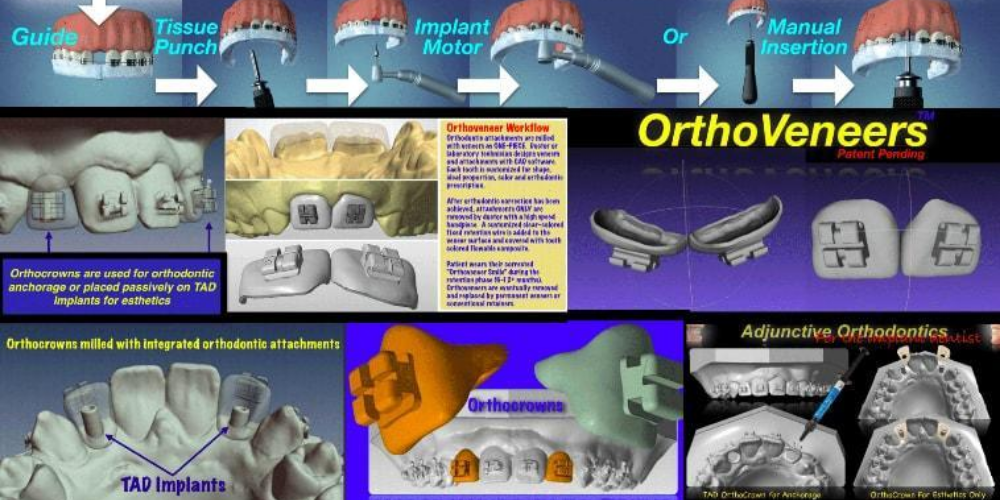
The OrthoVeneer System was developed before 3D printing materials were approved to be in the mouth for more than a day. In anticipation of technology catching up to the Orthoveneer idea we developed the system using yesterday’s FDA approved materials that had to be milled, not 3D printed. The 5-axis milling machines such as Cerec or Roland mills were very expensive. The time and cost to make each Orthoveneer or Orthocrown was substantial. In year 2018 several FDA approved materials have come to market. Also, the cost of in-house 3D printers are dramatically dropping in price. Orthodontists and Dentists will now or very soon treatment plan a patient’s adjunctive orthodontics and dental implant placement on a workstation, laptop or tablet computer. Complex cases that have broken down or missing teeth can be quickly treatment planned and printed on a 3D printer or milling machine.
The History of TADplant Concept & Its Development
The two emails (Pdfs files below) document part of the history of the TADplant concept and its development. When studying Implant Dentistry in Dr. Ed Mill’s AAID Maxi Course the idea of a provisional implant for lateral agenesis cases (Missing upper laterals) came to mind. The 2010 email illustrates a problem most orthodontists have when orthodontically preparing a younger patient for dental implants. The patient is often too young for a larger conventional dental implant at the end of their orthodontic treatment. Resin bonded bridges, Hawley retainers with pontic teeth and other removable types of retainers are the standard of care. In many cases the patient must wear retainers for 3, 5 or more years. Retainers break, are misplaced or, in most cases, not worn as instructed. The end result is the teeth adjacent to the implant sites relax or relapse as described in one of the emails below. Not only will the patient or parent have expense of dental implants, but additional orthodontic treatment may be required. Two dental implants, additional orthodontics and crowning can exceed $15,000. Our family’s legacy project is to find a more affordable solution.
Please review the emails below.
2015 Post on VuMedi Online Forum
Great VuMedi presentation!! Dr. Bahat’s four decades of experience treating complex dental implant complications related to NORMAL craniofacial remodeling we should have planned for before we placed implants. Thank you for sharing your experience with us!
I have been working on a solution related to the craniofacial changes in the “Esthetic Zone” you showcased in your presentation. As an implant trained orthodontist I have concluded the maxilla is a “moving target”. It is difficult to accurately predict the amount and timing of growth changes in the developing or aging maxilla.
Dr. Rolf Beherents, Editor of the AJO-DO in 1985 published his landmark growth study using the Bolton-Brush Growth Study Center longitudinal data base in the orthodontic literature (see ref. below).
In 1986 The Journal of Clinical Orthodontics Interviewed Dr. Beherents — Ref.: Dr. Rolf Behrents on Adult Craniofacial Growth, VOLUME 20 : NUMBER 12 : PAGES (842-847) 1986, LARRY WHITE, DDS, MSD
A few excerpts of the interview are quoted below:
“DR. WHITE Instead, you found changes were more general and greater than you expected?
DR. BEHRENTS Yes. We found that craniofacial growth did not stop in young adulthood, but was a continuous process even into later ages. The units of change were smaller, of course, but change in the craniofacial skeleton became the operational concept rather than termination of the process.
DR. WHITE How many of the original 6,000 participants were you able to find?
DR. BEHRENTS We were looking for orthodontically untreated individuals. Of the original 6,000 participants we were able to locate approximately 200 untreated individuals, and we ultimately examined 113. Most of them were still living in the Cleveland area.
DR. WHITE Did you find any general differences in the growth of men and women?
DR. BEHRENTS Sexual dimorphism seemed easier to understand in this adult sample, as opposed to an adolescent group, because for the most part these people had “dimorphed”; they were more or less finished developing characteristics of “maleness” or “femaleness”. Males, of course, were bigger to start with as adults, but they also grew more in later adulthood. Apart from size, male and female faces were different, and they grew differently. Males demonstrated a continuously decelerating curve of growth velocity. Females seemed to slow and then reaccelerate in their growth pattern. This seemed especially evident in their 20s and early 30s and may be related to other events in their lives, notably pregnancy. There is evidence to suggest that bone growth in pregnancy is a common occurrence, which seems to be seen in our study in the female craniofacial skeleton.
DR. WHITE Dr. Behrents, this work is one of the most significant and ambitious studies ever done on growth and development, and JCO thanks you immensely for sharing it with our readers.”
Reference: Dr. Beherents 1985 Mongraph 17, Growth in the Aging Craniofacial Skeleton, see page 87 RE: “Adult Conformational Adaptation”
Implant sites in the esthetic zone are affected EARLY by growth, development and maturation changes well into the 30s (ref. R. Beherents) and LATER by aging after 40 years of age (ref. O. Bahat). Again, I emphasize “The Maxilla is a moving target”. Maybe we should consider placing implants that can be later removed and replaced without destroying receptor sites. Surface enhancements to promote absolute osseointegration is the current thinking. Perhaps we should revisit earlier success models.
The following links are to other recent presentations on concepts described above. We are currently in clinical trials in my private practice and at Jacksonville University Orthodontic Department.
March 2015 San Francisco AO Meeting
https://www.dropbox.com/s/wvk2imt14e4mjsx/Evolution%20of%20the%20TAD%20Implant%20San%20Francisco%20Presentation.m4v?dl=0
TADplant and Orthoveneers
https://www.dropbox.com/s/ykzu80ew06qs520/MOV.Unitek%20Conference%20Call%2010%3A15%3A2014%202.m4v?dl=0
Please view my early VuMedi videos on the development of the placeholder/provisional TAD Implant that can be quickly inserted and later easily removed as the implant site remodels. TADplants can also be used for patients that can not NOW afford traditional “permanent” endosseous dental implants to slow down bone resorption from disuse atrophy. We hope to show that TADplants & Orthocrowns are “BAD”…bone anchor devices.
I have been invited to present results of the TADplant/Orthocrown project next February 2016 at the ICOI Winter Meeting in Miami Florida.
TADplant Patent Support References
1. Kalia, Ajit, Mini Screw Orthodontic Implant as Temporary Crown
Restoration to Replace Unilateral Missing Lateral Incisor post
Orthodontic Treatment, Journal of Oral Implantology, vol. XLI, No.
3, 2015, pp. 306-309.
2. Schulte, Michael, Temporary Anchorage Device (TAD) Supported
Pontics Prevent Bone Resorption in Young Growing Patients with
Missing Maxillary Lateral Incisors, https://cats.uthscsa.edu/pub
lished cats friendly.php?d=2964, Dec. 10, 2015, 2 pgs.
**The most significant article in Orthodontic literature by Dr. Cope below. Dr. Cope updated cases in this paper at the 2019 Los Angeles AAO Meeting. His miniscrew dental implant has been in place for 14 years. Proof of Dr. Cope’s 2003 Concept
**3. Cope et al., “Temporary replacement of missing maxillary lateral
incisors with orthodontic miniscrew implants in growing patients:
rationale, clinical technique, and long-term results’, JO Sep. 2014,
13 pgs. (Click LINK to highlighted copy with Dr. O’s comments)
4. Waugh, Robert, “CBCT and Barium Markers When Placing Tem
porary Implants: How can I use CBCT and barium markers when
placing temporary implants?” The Dentists’ Voice, 2012, 2 pgs.
Andrade et al., “Treatment for agenesis of maxillary lateral incisors:
a systematic review”. Orthodontics & Craniofacial Research, 2013,
9 pages.
5. Graham, John W. “Temporary Replacement of Maxillary Lateral
Incisors with Miniscrews and Bonded Pontics’, Journal of Clinical
Orthodontics, vol. 41, Issue 6, 2007, pp. 321-325.
6. Kavedia et al., “Agenesis of maxillary lateral incisors: a global
overview’. Orthodontics: the art and practice of dentofacial
enhancement, UMKC Dental Library Periodical, vol. 12, No. 4.
2011, pp. 296-317.
7. Uribe et al., “Cone-beam computed tomography evaluation of
alveolar ridge width and height changes after orthodontic space
opening in patients with congenitally missing maxillary lateral
incisors’. American Journal of Orthodontics and Dentofacial Ortho
pedics, vol. 144, Issue 6, Dec. 2013, pp. 848-859.
8. Kokich et al., “Congenitally missing maxillary lateral incisors:
Restorative replacement’. American Journal of Orthodontics and
Dentofacial Orthopedics, Apr. 2011, vol. 139, Issue 4, pp. 435-445.
9. Pini et al., “Congenitally Missing Maxillary Lateral Incisors: update
on the Functional and Estehtic Parameters of Patients Treated with
Implants or Space Closure and Teeth Recontouring”. The Open
Dentistry Journal, 2014, 10 pages.
10. Kokich, Vince, Jr., “Early Management of Congenitally Missing
Teeth’. Seminars in Orthodontics, 11, pp. 146-151.
11. Flanagan, Dennis, “Fixed Partial Dentures and Crowns Supported
by Very Small Diameter Dental Implants in Compromised Sites”.
Implant Dentistry, vol. 17. No. 2, pp. 182-191.
12. Kinzer et al., “Managing Congenitally Missing Lateral Incisors,
Part II: Tooth-Suported Restorations”, Journal of Esthetic and
Restorative Dentistry, vol. 17, 2005, pp. 76-84.
13. Kinzer et al., “Managing Congenitally Missing Lateral Incisors,
Part III: Single-Tooth Implants”, Journal of Esthetic and Restorative
Dentistry, vol. 17, 2005, pp. 202-210.
14. Gurgel et al., “Mini-Implants as Provisional Anchorage for the
Replacement of Missing Anterior Teeth: A Clinical Report’. The
Journal of Prosthetic Dentistry, 112.2014, pp. 706-709.
15. Giannetti, “Mini-implants in growing patients: a case report’.
Pediatric Dentristy, vol. 32, Issue 3, 2010, pp. 239-246.
16. Mazor et al., “Mini-Implants to Reconstruct Missing Teeth in
Severe Ridge Deficiency and Small Interdental Space: A 5-Year
Case Series’. Implant Dentistry, vol. 13, No. 4, 2004, pp. 336-341.
17. Bhalla et al., “Miniscrew design and bone response: Defining a
correlation’. Scientific Innovation, vol. 14, 2013 13 pages.
18. Ciarlantini et al., “Miniscrew-retained pontics in growing patients:
a biological”, Journal of Clinical Orthodontics, vol. 46, Issue 10,
Oct. 2012, pp. 638-640.
19. Gleizny’s et al., “New approach towards mini dental implants and
Small-diameter implants: an option for long-term prostheses’.
Stomatologija Baltic Dental and Maxillofacial Journal, vol. 14, No.
2, 2012, pp. 39-45.
20. Keller, G. William, “Temporarily Replacing Congenitally Missing
Maxillary Lateral Incisors in Teenagers Using Transitional
Implants’, Dental Tribune, Jul.-Sep. 2003, No. 2, vol. 1, 2 pages.
Key References supporting the TADplant System because of Normal Bone Maturation and Aging Changes
21. https://tadplant.com/semipermanent-replacement-of-missing-maxillary-lateral-incisiors__-with-tad/
22. ** A Novel Bone Preservation Study (2015 by Melsen, B) using Mini Screws Link >> https://tadplant.com/alveolar_bone_preservation_subsequent_to_miniscrew/
23. https://tadplant.com/jason-cope-tad-14yrs-in-max-arch/
25. Mendleson, Bryan and Wong, Chin-Ho, Changes in the Facial Skeleton with Aging: Implications and Clinical Applications in Facial Rejuvenation, Aesthetic Plastic Surgery, 36 (4): 753-760. DOI: 10.1007/s00266-012-9904-3
26. Bahat, Oded., Dynamic Craniofacial Changes Associated with Aging. Vumedi, Jul 21, 2015.
27. Ouellette, Paul, Ouellette, Jonathan, Ouellette, Jason, Are Occlusion Concepts Valid in an Asymmetric World? DentalXp, Atlanta, Ga, Nov 2013.
28. Zachrisson, Bjoren, Important Aspects of Long-Term Stability, JCO, Volume 1997, Sep (562-583)
29. Sharma, Padmaja, Arora, Ankit, Valiathan, Age Changes of Jaws and Soft Tissue Profile, The Scientific World Journal, Volume 2014, Article ID 301501, 7 Pages
30. Yan, Gu, McNamara, James A., Cephalometric Superimpositions
A Comparison of Anatomical and Metallic Implant Methods, Angle Orthodontist, Vol 78, No 6, 2008, Pages 967-976.
31. Flanagan, Dennis, The Case for Smaller Diameter, Journal of Oral Implantology, Letter to the Editor, Dec 2016 2016;42(6):517-517.
32. Wilmes, Bennedict et al., Mini-Implant-Supported Temporary Pontics, Journal of Clinical Orthodontics, July 2014, Pgs. 422-429.
33. Gowri, S and Vasu, M., Temporary Anchorage Devices in Orthodontics, Annuals and Essences in Dentistry, Vol 1 Issue 1, July-Sept 2009
34. Singh, K, Kumar, D, Jaiswal, R and Bansal, A, Temporary anchorage devices – Mini-implants, National Journal of Maxillofacial Surgery, Jan-June; 1(1): 30-34
35. Pini, Nubia, Luciana, Marchi and Correa, Pascotto, Congenitally Missing Maxillary Lateral Incisors: Update on the Functional and Esthetic Parameters of Patients Treated with Implants or Space Closure and Teeth Recontouring, The Open Dentistry Journal, 2014, 8, 289-294.